
In this blog series we are going to do a deep dive into the 2021 E/M Changes. During the series I will be referring to the official guidelines from the AMA. Click the link below to download a copy.
https://www.ama-assn.org/system/files/2019-06/cpt-office-prolonged-svs-code-changes.pdf
In the last post we talked about how time is going to change the way you level your office/outpatient visits come 2021. Today we are going to dig into how prolonged services will change as well.
New Prolonged Service Code
If you want an early Christmas present click on the link above and go to page 9. Starting from page 9 until the end of the document is a preview of of the 2021 CPT-4 code book. If you are as big of a coding geek as I am you will be able to imagine how much my dorky coder heart swooned when I saw an actual preview of the 2021 CPT book in this document. But I digress. If you will refer to the last two pages, you will see that the AMA has created a brand new CPT code to report prolonged service codes. That code is 99XXX. Yep weird huh? Below are some guidance on how you will use 99XXX in 2021.
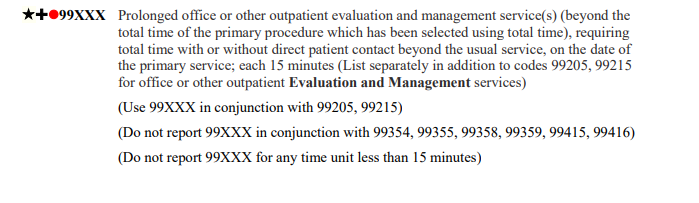
Report 99XXX with 99205 and 99215 only.
The guidance in the parenthesis tells us that we can only report 99XXX with EM codes 99205 and 99215. Do not report 99XXX with any other codes.
Do Not Report 99XXX for Less Than 15 Minutes
The guidance in parenthesis also instructs us to not report prolonged services for less than 15 mins. In those cases report only 99205 or 99215.
Prolonged Service Time Table
The AMA created the handy table below to make it easy to report office/outpatient prolonged services.
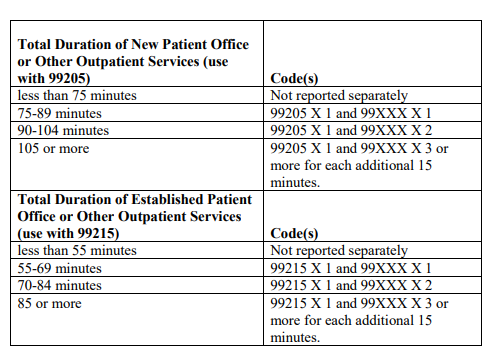
I would like to point out a bonus Christmas present. Notice on the table it states that if you document 75-89 minutes for a new patient you can report 99205 with 99XXX x 1 unit. Well that is very interesting since the time range (see table below) for 99205 will be 60-74 minutes. Let that sink in. The AMA is saying that if you 75 minutes with a new patient you can bill 99205 and also 1 unit of 99XXX. That is literally only one minute more than the time range for the code 60-74 minutes. You are welcome! Note that the same is true with established patient visits. If you document 55 minutes with an established patient you get to bill 99215 plus 99XXX x 1.
| CPT-4 Code | Time Range |
| 99205 | 60-74 |
| 99215 | 40-54 |
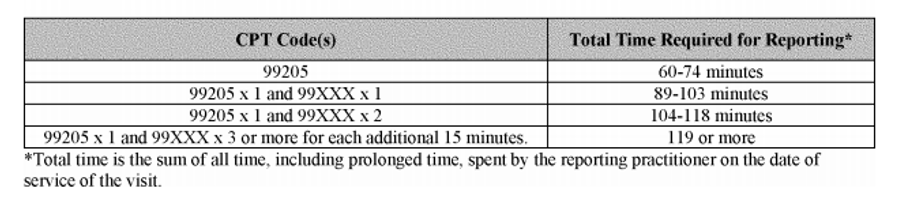
Before you celebrate too much let’s ask the most important question. Will CMS follow suit with their time calculations? Don’t bet on it. According to the CMS Proposed rule that was released on 8/17/2020 they are not going to be following the AMA’s lead on this. If you compare the CMS tables below to the AMA tables at the beginning of this post you will see there is a difference in the way the CMS sees the threshold times for 99XXX. Notice that for 99205 x 1 unit of 99XXX the time is 75-89 minutes for the AMA but it is 89-103 minutes for CMS. Since this is the “proposed rule” it is subject to change. Once the final rule comes out in November we will know for sure.

The next post will be all about medical decision making (MDM). We will talk about how it is changing for 2021 and how it will be used to level an office visit in 2021.
